
Release time :2024-07-09
Source:support@yingchitech.com
Scan:715
Clinical Support Department of Shenzhen Yingchi Technology Co.,Ltd.
01 Safety of TMS in children
02 TMS treatment of autism spectrum disorder
03 TMS treatment of tourette syndrome
04 TMS treatment of attention-deficit/hyperactivity disorder
05 TMS treatment of treatment resistant disorder
06 TMS treatment of generalized anxiety disorder
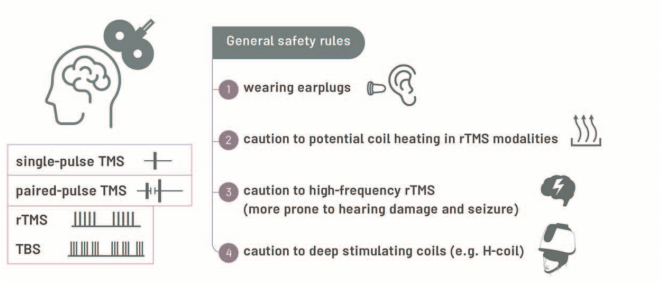
In children and adolescents, adverse reactions and side effects of transcranial magnetic stimulation (TMS) are similar to those reported in adults and are mild and transient in currently used protocols.
The results of safety-related studies published in the last two years suggest that TMS is safe and well tolerated in children and adolescents if safety rules, including exclusion criteria, are followed.
In TMS studies, patients with epilepsy or a history of previous seizures should be considered exclusion criteria unless epilepsy is the treatment objective. Earplugs should be used in TMS studies to prevent potential hearing loss.
We still need systematic studies on appropriate targeting methods and stimulation doses for noninvasive brain stimulation in children, as well as long-term safety.
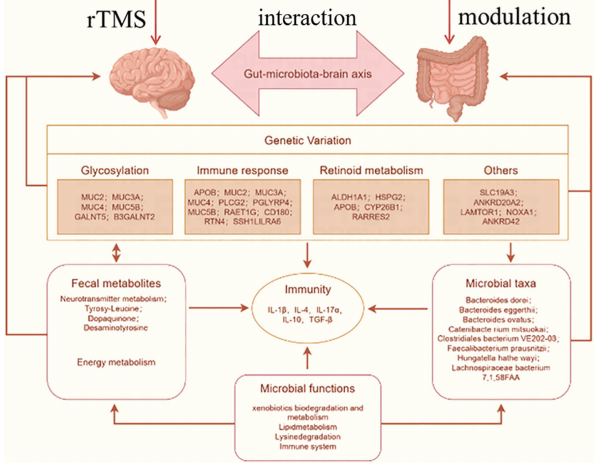
New evidence suggests a potential link between the development of autism spectrum disorders and gut-brain axis disorders. Repetitive transcranial magnetic stimulation (rTMS) is a non-invasive means of diagnosis and treatment that has shown positive results in a variety of psychiatric disorders; However, its efficacy in the treatment of ASD and its concomitant gastrointestinal effects, especially on the gut-brain axis, are unknown.
This review delves into the use of transcranial magnetic stimulation in the treatment of ASD and explores the interaction between rTMS and the gut microbiota in children with ASD, with a focus on the gut-brain axis. In addition, the combined application of transcranial magnetic stimulation and gut microbiota modulation is deeply investigated as a targeted treatment for ASD based on the latest literature. Potential synergistic effects of rTMS and gut microbiota interventions are also highlighted, the underlying mechanisms are described, and potential treatment strategies for specific ASD patients are proposed.
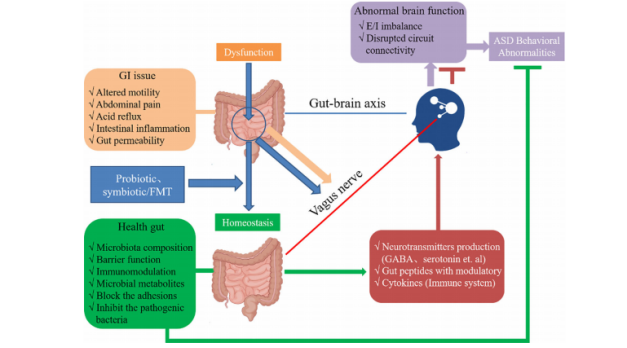
(1) ASD core symptoms, GI symptoms and intestinal flora changes interact and influence each other.
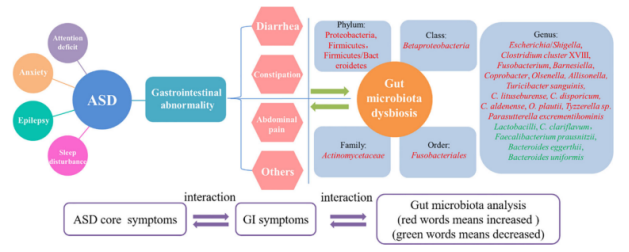
(2) rTMS combined with intestinal microbiota regulation can play a dual regulatory role and contribute to the treatment of ASD.
Sleep difficulties may coexist with autistic traits and are frequently reported in children diagnosed with autism. Sleep difficulties may affect neurodevelopment, cognitive, and behavioral functioning in children with autism. Interventions such as repetitive transcranial magnetic stimulation (rTMS) target abnormal neural structures underlying autistic traits and sleep difficulties in children and may therefore have beneficial effects.
Application of rTMS in comorbid sleep disorders in ASD
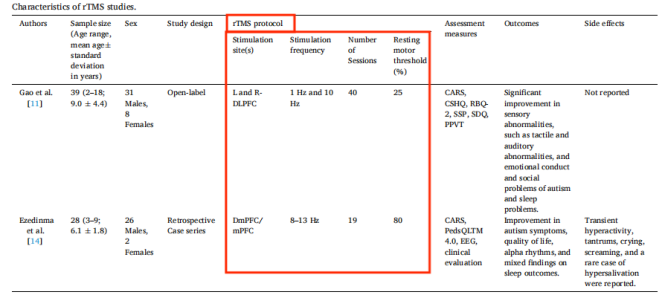
① (Gao et al.) A combination of low (1Hz) and high (5Hz) frequency rTMS was applied to the left and right dorsolateral prefrontal cortex (DLPFC), 5 times a week for 1 week, with a 4-week interval between two treatments.
② (Ezedinma et al.) The individual alpha peak frequency based on resting-state EEG measurement was used as the individual rTMS stimulation frequency, that is, individualized high-frequency stimulation of the dorsomedial prefrontal cortex (dmPFC) and/or the medial parietal cortex (mPC).
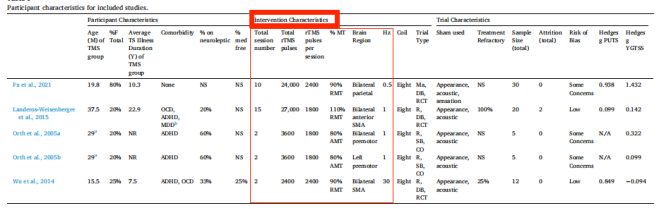
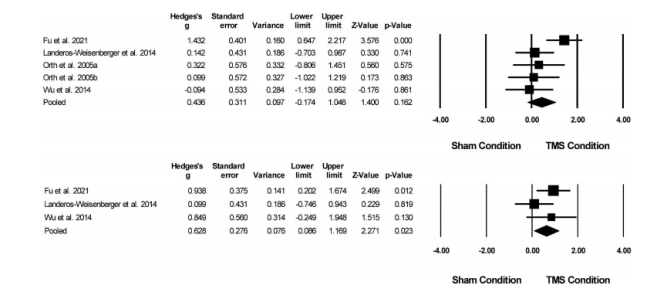
This meta-analysis examines the effect of transcranial magnetic stimulation on reducing tic severity in patients with Tourette Syndrome (TS) and explores the effect of transcranial magnetic stimulation on reducing the severity of premonitory urges—the first line of evidence for TS Main mechanisms of treatment. The results showed that transcranial magnetic stimulation did not significantly reduce the severity of convulsions (P = 0.16), but the severity of aura impulses was moderately reduced (p<0.02). In trials with larger sample sizes and a predominantly female population, transcranial magnetic stimulation was more effective in treating tic severity.
(1) Treatment parameters and other characteristics
(2) Effect of TMS on tic severity

To investigate the effect of repetitive transcranial magnetic stimulation (rTMS) on ADHD.
Randomized sham-controlled trials (RCTs) were identified from primary databases from January 1990 to January 2023. The primary outcome was improvement in total ADHD symptoms. Subgroup analyses focused on the efficacy of rTMS targeting different brain regions. Secondary outcomes were the associations of rTMS with improvement in different ADHD symptoms.
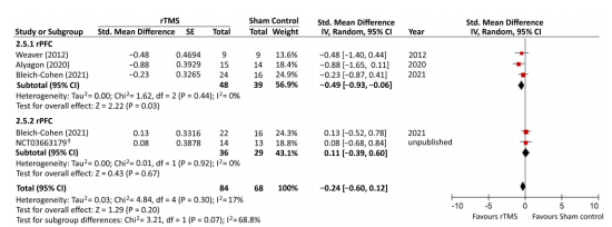
A meta-analysis of 6 randomized controlled trials involving 169 participants showed no difference in total ADHD symptoms between rTMS-treated and sham-controlled groups (SMD = -0.24, p = 0.17). Subgroup analysis showed that rTMS targeting the right prefrontal cortex (rPFC) was more effective than sham control (SMD = -0.49, p = 0.03), but targeting the left prefrontal cortex (lPFC) was less effective (SMD = 0.01, p = 0.67). rTMS treatment was associated with improvements in inattention symptoms (SMD = -0.76, p = 0.0002), but not in hyperactivity (p = 0.86), impulsivity (p = 0.41), and depression (p = 0.95).
The results of this study only support the therapeutic effect of rTMS targeting rPFC on ADHD symptoms (especially inattention), but not the therapeutic effect of targeting IPFC. Further large-scale randomized sham-controlled trials are needed to verify this conclusion.
① Stimulation target: right dorsolateral prefrontal lobe, Intensity: 120% rMT, Frequency: 1Hz, Stimulation time: 60s, Interval time: 30s, Number of repetitions: 6 times, Total number of pulses: 360.
② Stimulation target: left dorsolateral prefrontal lobe, Intensity: 120% rMT, Frequency: 20Hz, Stimulation time: 2s, Interval time: 4s, Number of repetitions: 30 times, Total number of pulses: 1200.
Once a day, five days a week, for a total of 36 treatments.
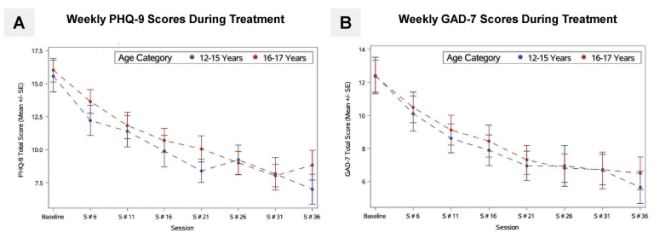
Improvements in depression and anxiety scores continued throughout treatment. There was no significant plateau in improvement in either score in either group. It is important to note that statistical analysis did not find any significant differences in treatment outcomes between the 12-15 and 16-17 age groups on continuous or categorical measures.
Stimulation target: right dorsomedial prefrontal cortex (about 2 cm outside Fz); Intensity: 120% rMT (lower limbs); Frequency: 1Hz; Stimulation time: 10min; Total number of pulses: 600.
Course of treatment: ten days (5 days/week), 3 times a day, ≥60min interval between two times
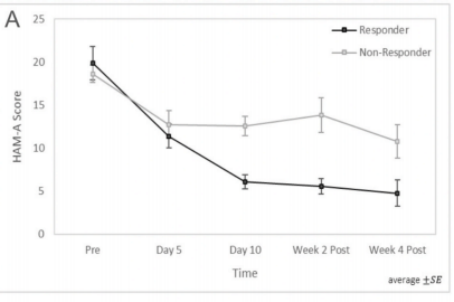
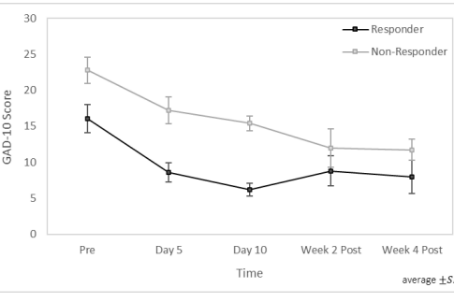
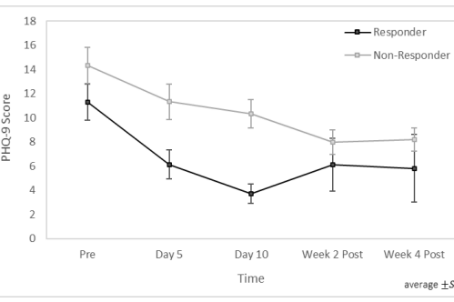
Research shows that 1Hz rTMS stimulation of the dorsomedial prefrontal cortex is safe and well-tolerated in adolescents/young adults with generalized anxiety disorder (GAD). The anti-anxiety effect is obvious - 50% of patients achieved relief after 10 days, and 69% of patients met the response criteria of the Hamilton Anxiety Rating Scale (HAM-A). The adjuvant treatment effect on depressive symptoms and suicidal tendencies is also significant.

This content is organized by the Clinical Support Department of Shenzhen Yingchi Technology Co.,Ltd. Criticisms and corrections are welcome. For reprint, please indicate the source.






